

Tennis elbow is commonly called lateral epicondylitis, lateral epicondylalgia, or lateral epicondylitis depending on whether inflammation is present or not. Tennis elbow (lateral epicondylitis) problems usually occur in persons 35 years of age or older and in those who use a great deal of wrist flexion and extension in their occupations or activities, requiring wrist stabilization in slight extension Symptoms include pain in the common wrist extensor tendons along the lateral epicondyle and HR joint with gripping activities. Activities requiring firm wrist stability, such as the backhand stroke in tennis, or repetitive work tasks that require repeated wrist extension, such as computer keyboarding or pulling weeds in a garden, can stress the musculotendinous unit and cause symptoms.

The most frequent location of involvement is in the musculotendinous junction of the extensor carpi radialis brevis although the extensor communis is also involved in many patients. The injury results in a sensory loss in the forearm; it is usually the result of forced elbow hyperextension or repeated pronation (e.g., excessive screwdriver, backhand tennis strokes) and may be misdiagnosed as tennis elbow.
Symptoms also occur when the annular ligament is stressed. Positive tests of provocation include palpation tenderness on or near the lateral epicondyle, pain with resisted wrist extension performed with the elbow extended, pain with resisted middle finger extension performed with the elbow extended, and pain with passive wrist flexion with the elbow extended and forearm pronated. It appears to be a degenerative condition in which the tendon has failed to heal properly after repetitive microtrauma injury.
there may be signs of inflammation followed by the formation of granulation tissue and adhesions. With repetitive trauma, fibroblastic activity and collagen weakening occur. Recurring problems are seen because the resulting immobile or immature scar is pre-damaged when returning to activities before there is sufficient healing or mobility in the surrounding tissue. Hypersensitivity over the radial and ulnar nerves has been reported to occur in women with lateral epicondylalgia, indicating a possible link between mechanical irritation and nerve sensitization.
Etiology of Tennis elbow
The most common cause of epicondylalgia is excessive repetitive use or eccentric strain of the wrist or forearm muscles. The result is microdamage and partial tears, usually near the musculotendinous junction when the strain exceeds the strength of the tissues and when the demand exceeds the repair process. Initially,there may be signs of inflammation followed by the formation of granulation tissue and adhesions. With repetitive trauma, fibroblastic activity and collagen weakening occur. Recurring problems are seen because the resulting immobile or immature scar is pre-damaged when returning to activities before there is sufficient healing or mobility in the surrounding tissue. Hypersensitivity over the radial and ulnar nerves has been reported to occur in women with lateral epicondylalgia, indicating a possible link between mechanical irritation and nerve sensitization.
Special tests for Lateral Epicondylitis
1) Cozen’s Test for Lateral Epicondylitis
The patient’s elbow is stabilized by the examiner’s thumb, which rests on the patient’s lateral epicondyle. The patient is then asked to actively make a fist, pronate the forearm, and radially deviate and extend the wrist while the examiner resists the motion. Sudden severe pain of the lateral epicondyle of the humerus is a positive sign for this test. The epicondyle may be palpated to indicate the origin of the pain.

2) Mill’s Test for Lateral Epicondylitis
While palpating the lateral epicondyle, the examiner passively pronates the patient’s forearm, flexes the wrist fully, and extends the elbow. Pain over the lateral epicondyle of the humerus indicates a positive test. This maneuver also puts stress on the radial nerve and, in the presence of compression of the radial nerve, causes symptoms similar to those of tennis elbow. Sometimes Electrodiagnostic studies help differentiate the two conditions.
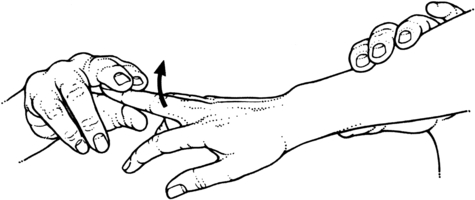
3) Maudsley’s Test for Lateral Epicondylitis
The examiner resists the extension of the third digit of the hand distal to the proximal interphalangeal joint, stressing the extensor digitorum muscle and tendon. A positive test is indicated by pain over the lateral epicondyle of the humerus.
This all test should be done under the observation of experienced instructor or Physiotherapist. strongly avoid such test performing by self. it can cause you more harm then you thaught. because such special test is provocation test which meant to provoke the pain in bearable amount. by performing without experience can worsen the condition. information here is only for the informative purpose mostly for physiotherapy students and common person.
Structural and Functional Impairments
- Gradually increasing pain in the elbow region after the excessive activity of the wrist and hand
- Pain when the involved muscle is stretched or when it contracts against resistance
- Decreased muscle strength and endurance for the demand
- Decreased grip strength, limited by pain
- Tenderness with palpation at the site of inflammation, such as over the lateral or medial epicondyle, head of the radius, or in the muscle belly
Activity Limitations and Participation Restrictions
- Inability to participate in provoking activities, such as racket sports, throwing, or golf.
- Difficulty with repetitive forearm/wrist tasks, such as sorting or assembling small parts, typing on a keyboard or using a computer mouse, gripping activities, using the hammer, turning a screwdriver, shuffling papers, or playing a percussion instrument.
Comments
Post a Comment